
Case-Report | DOI: https://doi.org/10.31579/2578-8868/142
Department of Neurosurgery, National Neuroscience Institute (NNI), Singapore
*Corresponding Author: Eng Tah Goh, Department of Neurosurgery, National Neuroscience Institute (NNI), Singapore
Citation: Goh ET., Keong NCH. (2020) Rupture of a Previously Undiagnosed Anterior Communicating Artery Aneurysm following External Lumbar Drainage in a Patient with Normal Pressure Hydrocephalus: A Case Report. J. Neuroscience and Neurological Surgery. 6(5); DOI:10.31579/2578-8868/142
Copyright: © 2020 Eng Tah Goh, This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 19 October 2020 | Accepted: 28 October 2020 | Published: 05 November 2020
Keywords: aneurysm; hydrocephalus; lumbar drainage; subarachnoid haemorrhage
Background and importance:
Both asymptomatic unruptured intracranial aneurysms (AUIA) and idiopathic normal pressure hydrocephalus (NPH) have been found in the elderly population to increase in incidence with advancing age. In NPH, external lumbar drainage (ELD) is a gold standard and widely accepted low-risk procedure for supplemental testing of CSF responsiveness and suitability for surgical intervention. Herein, we reported the first case of aneurysmal subarachnoid haemorrhage (SAH) as a cause of neurological decline following ELD for the testing of patients with NPH.
Clinical Presentation:
A 65-year-old gentleman with probable NPH was admitted for supplemental testing using ELD. He had demonstrated CSF responsiveness as evidenced by improving Tinetti score. Unfortunately, on the third day of post-insertion, his GCS deteriorated from 15 to 3 due to rupture of a previously undiagnosed anterior communicating artery (Acom) aneurysm. He underwent left frontal external ventricular drain in an emergency setting and his GCS improved to E1VtM4. After frank discussion with his family, we proceeded with craniotomy and clipping of the aneurysm. However, his neurological recovery remained poor post-operatively and he had eventually undergone tracheostomy and ventriculo-peritoneal shunt.
Conclusion:
As SAH is also a known trigger of secondary NPH, there may be a critical role for screening of AUIA prior to ELD for NPH. The characterization of this risk would then allow for a full discussion of surgical or endovascular treatment options for AUIA, as well as the risk-benefit ratio of proceeding with supplemental testing and intervention for NPH.
Background and Importance
Both asymptomatic unruptured intracranial aneurysms (AUIA) and normal pressure hydrocephalus (NPH) have been found in the elderly population to increase in incidence with advancing age. In NPH, external lumbar drainage (ELD) is a gold-standard and widely accepted low-risk procedure for supplemental testing of CSF responsiveness. Herein, we reported the first case of aneurysmal subarachnoid haemorrhage (SAH) as a cause of neurological decline following ELD for the testing of NPH. This report illustrates how a rare coexistent AUIA complicated the management of NPH after ELD.
Clinical Presentation
A 65-year-old man was re-referred to the neurosurgery for re-evaluation of NPH. 2 years prior to this new referral, he had been thought to fulfil the diagnostic criteria for probable NPH as he was having 4 years of gait, balance and cognitive symptoms. His imaging (figure 1) confirmed ventriculo-megaly and supplemental testing using ELD had demonstrated responsiveness to CSF withdrawal. However, at that stage he declined intervention. He re-presented due to neurological decline over several months.
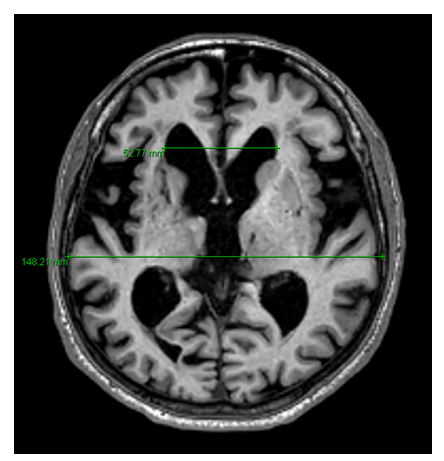
Figure 1: MRI Brain demonstrating Evans’ index of 0.30
In addition to hypertension and dyslipidaemia, he had a recent history of colon cancer, for which he underwent laparoscopic anterior resection 4 months prior to re-referral. Fortunately, he was able to make a satisfactory recovery despite complex post-operative complications (mainly ileus and sepsis). Whilst he had been able to return to his normal work, his gait tolerance had reduced to approximately 5 metres before he became stuck or developed shuffling. He had also developed urinary incontinence. Following our discussion, he wished to consider surgical intervention if he was still responsive to CSF diversion. Hence, he was duly admitted for a repeat ELD.
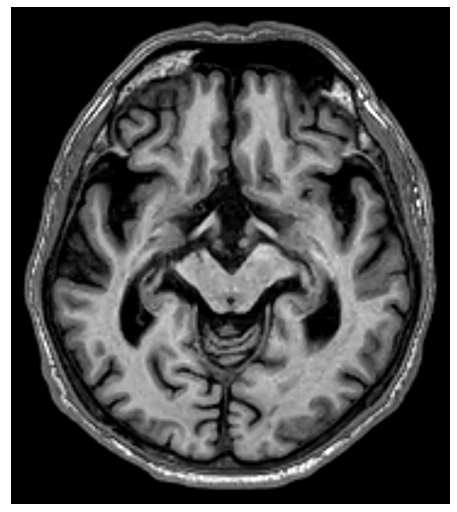
Pre-ELD, he scored 18/28 upon Tinetti assessment. His Mini Mental State Examination (MMSE) had improved to 29/30 since his previous testing (25/30). No vascular imaging was performed to screen for AUIAs but the T1-weighted imaging (figure 2) was unremarkable. He underwent an ELD insertion, incorporating a 30-ml CSF tap test, and his immediate post-insertion course was uneventful.
His CSF was found to be clear and colourless. By day 3, his Tinetti score had improved to 22/28 (see table 1).

On the night of the third day post-ELD, he exhibited a sudden drop of GCS to 3, with bilateral pupillary dilatation. He was noted to be hypertensive and tachycardic. At this time, as he had already reached the desired CSF drainage target for the day, the ELD was clamped as per protocol. However, it was immediately unclamped upon neurological deterioration - heavily blood-stained CSF was drained. Following resuscitation, he was transferred for a CT brain (figure 3) - which revealed extensive SAH.

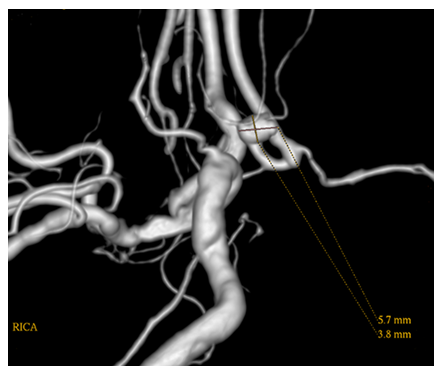
He underwent an emergency replacement of the ELD with a left frontal external ventricular drain (EVD). Post-operatively, his GCS improved to E1VtM4. An urgent cerebral angiogram demonstrated an anterior communicating artery (Acom) aneurysm with a small daughter sac (see figure 4).
Despite clipping of aneurysm and maximal neurointensive care, his neurological recovery remained poor. He eventually underwent a tracheostomy and a ventriculo-peritoneal shunt before discharge. He passed away at 1-year post-ictus.
Discussion
This case illustrates how the rupture of a previously unknown AUIA complicated the further management of NPH. Although the coexistence of both diagnoses is rare, studies have suggested that the risk of both conditions occurring increase with age. Previously published vascular work from our unit has shown that the overall prevalence of AUIA in a Southeast Asian population was 3.5% and an increasing trend was found with advancing age.[1] Similarly, idiopathic NPH has also been demonstrated to increase in prevalence among those over 65 years old. [2-4]. Currently, there is no clinical data to estimate the prevalence of AUIA specifically amongst patients with NPH.
CSF drainage is critical to the management of both aneurysmal SAH and NPH. In SAH, ELD may confer some neurological advantages in the management of SAH, such as reduction of vasospasm and the need for longer-term CSF diversion. [5] In NPH, ELD is a gold-standard supplemental test because it has the highest sensitivities and positive predictive values in the published literatures. [6-9].
Aneurysmal re-rupture is a known complication of ELD and EVD. [10,11]. It is hypothesized that a sudden-change transmural pressure after CSF drainage may provoke aneurysmal re-rupture. Secondly, in cases where thrombus at the dome of the ruptured aneurysm is adherent to clot extending from the subarachnoid space into adjacent parenchyma, displacement of brain tissue following a drop in CSF pressure may provoke re-rupture. Such hypotheses, though valid in the context of SAH, would not be applicable in this case. Unlike aneurysmal SAH, intracranial pressure in NPH typically remains at low-to-normal levels despite intervention. There was also no suggestion of either a history consistent with sentinel SAH or evidence of occult SAH detectable on MRI pre-ELD. However, the aneurysm did demonstrate morphology favouring higher risk of rupture with the presence of daughter sac. It is therefore likely that the SAH that occurred during the ELD represented the first spontaneous rupture of the aneurysm.
In the published guidelines, [9,12-14] management of NPH has focused upon its idiopathic variety, whilst guidance for patients with significant comorbidities or secondary NPH has been less available. A more recent taskforce report has addressed the former but does not include consideration of AUIAs in this population. [15]
Intracranial aneurysms are known to cause hydrocephalus due to mechanical obstruction at certain anatomical locations, [16] but aneurysmal SAH is also a well-recognized cause for secondary NPH [17] - the vast majority would be non-obstructive. The screening for aneurysms in NPH, however, is not part of routine clinical practice. Screening in the form of a CTA or MRA could be easily incorporated into the workflow for NPH patients to prevent such avoidable morbidity (see Figure 5).

Appropriate management options could then be offered to patients who are found to have both an AUIA and NPH syndrome co-existing prior to NPH testing. We have subsequently adopted this workflow into our NPH programme, which has since successfully identified such cases for enhanced discussion regarding specific risks, benefits and expectations of managing both AUIA and NPH concurrently.
This case illustrates how the rupture of a previously unknown AUIA complicated the further management of NPH. Although the coexistence of both diagnoses is rare, studies have suggested that the risk of both conditions occurring increase with age. Previously published vascular work from our unit has shown that the overall prevalence of AUIA in a Southeast Asian population was 3.5% and an increasing trend was found with advancing age.[1] Similarly, idiopathic NPH has also been demonstrated to increase in prevalence among those over 65 years old.[2-4]. Currently, there is no clinical data to estimate the prevalence of AUIA specifically amongst patients with NPH.
CSF drainage is critical to the management of both aneurysmal SAH and NPH. In SAH, ELD may confer some neurological advantages in the management of SAH, such as reduction of vasospasm and the need for longer-term CSF diversion.[5] In NPH, ELD is a gold-standard supplemental test because it has the highest sensitivities and positive predictive values in the published literatures. [6-9].
Aneurysmal re-rupture is a known complication of ELD and EVD. [10,11]. It is hypothesized that a sudden-change transmural pressure after CSF drainage may provoke aneurysmal re-rupture. Secondly, in cases where thrombus at the dome of the ruptured aneurysm is adherent to clot extending from the subarachnoid space into adjacent parenchyma, displacement of brain tissue following a drop in CSF pressure may provoke re-rupture. Such hypotheses, though valid in the context of SAH, would not be applicable in this case. Unlike aneurysmal SAH, intracranial pressure in NPH typically remains at low-to-normal levels despite intervention. There was also no suggestion of either a history consistent with sentinel SAH or evidence of occult SAH detectable on MRI pre-ELD. However, the aneurysm did demonstrate morphology favouring higher risk of rupture with the presence of daughter sac. It is therefore likely that the SAH that occurred during the ELD represented the first spontaneous rupture of the aneurysm.
In the published guidelines, [9,12-14] management of NPH has focused upon its idiopathic variety, whilst guidance for patients with significant comorbidities or secondary NPH has been less available. A more recent taskforce report has addressed the former but does not include consideration of AUIAs in this population. [15]
Intracranial aneurysms are known to cause hydrocephalus due to mechanical obstruction at certain anatomical locations, [16] but aneurysmal SAH is also a well-recognized cause for secondary NPH [17] - the vast majority would be non-obstructive. The screening for aneurysms in NPH, however, is not part of routine clinical practice. Screening in the form of a CTA or MRA could be easily incorporated into the workflow for NPH patients to prevent such avoidable morbidity (see Figure 5).
AUIAs and NPH have both been found to increase in incidence with advancing age. The convergence of such cohorts has not been well-recognized in neurosurgical practice. As SAH is also a known trigger of secondary NPH, there may be a critical role for screening of AUIA prior to ELD. The characterization of this risk would then allow for a full discussion of treatment options for AUIA, as well as the risk-benefit ratio of proceeding with supplemental testing and intervention for NPH.
Verbal consent was obtained from the patient’s next of kin prior to this case report because this patient has no mental capacity for decision making. This was documented in the patient’s case notes.
This case report was presented as an e-poster in the 2019 World Federation of Neurosurgical Societies (WFNS) Special World Congress on 9-12September 2019 in Beijing, China.
The authors have no personal, financial, or institutional interest in any of the drugs, materials, or devices described in this article.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
